



By: Susan Berkman, MS, RD, LD, CDE, and Bethany Panchal, MD
The Ohio State University Wexner Medical Center Department of Family Medicine
Reprinted from the summer 2019 issue of The Ohio Family Physician.
Intro
Gestational Diabetes Mellitus (GDM) is a leading cause of complication in U.S. pregnancies, affecting approximately 7% of pregnant women. The incidence of GDM is higher in minority populations, especially in women of Hispanic, African, Asian, Native American, and Pacific Island decent. Although this disease can lead to many serious complications for both mother and baby, if monitored and treated appropriately, most women can go on to have uncomplicated deliveries and healthy infants. It is important to evaluate all stages of a woman’s life to assess for risk factors and to develop a plan to prevent progression of disease. Women who have been diagnosed with GDM are up to nine times more likely to develop Type 2 Diabetes Mellitus (T2DM) later in life. Lifestyle factors, including adopting a healthy diet and regular exercise are essential components to address in women, and will play a large role in contributing to insulin sensitivity and healthy blood sugar control in many individuals. No matter the stage of life, women can benefit from making their blood sugar control a priority.
Pre-Pregnancy
For the woman who is trying to become pregnant, it is important to implement healthy lifestyle habits early. Being at a healthy weight, participating in regular exercise, and having regular follow-ups with a family physician, other health care professional, and/or an obstetrician/gynecologist are integral in ensuring a woman enters into a healthy pregnancy. To prevent insulin resistance prior to pregnancy, it is recommended to follow a dietary pattern rich in fruits and vegetables, whole grains, lean proteins, and low-fat dairy products, while limiting certain nutrients, such as sugar, saturated and trans fats, and excess alcohol. It is recommended that all women of child-bearing age take a prenatal vitamin to provide nutrients essential for early fetal development, especially folic acid.
Exercise promotes insulin sensitivity and it is recommended that women participate in at least 150 minutes per week of moderate-intensity physical activity or 75 minutes per week of vigorous-intensity physical activity. Maintaining a healthy body mass index (BMI) (18 – 25 kg/m²) is integral as excess body fat leads to insulin resistance.
During Pregnancy
Due to the placenta’s production of hormones, all women are at higher risk for becoming insulin resistant during pregnancy. While diagnostic and treatment criteria for GDM is still being debated, the American College of Obstetrics and Gynecology (ACOG) and the American Diabetes Association agree that all pregnant women should be screened utilizing some form of a glucose tolerance test between weeks 24-28 of gestation. In certain high-risk populations, earlier blood glucose screening may be indicated. If a diagnosis of GDM is confirmed, management consists minimally of nutrition therapy, physical activity, and glucose monitoring. If this does not appropriately control blood sugar, medications are added. Insulin continues to be the first choice for treatment of uncontrolled glucose in pregnancy but if this is not feasible for any reason (patient preference, ability, cost, etc.), metformin is the second line therapy.
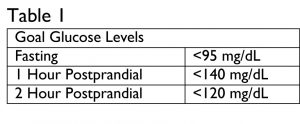
Women who have been diagnosed with GDM are required to check their blood sugars at least 4 times daily, 1 fasting and 3 post prandial, and should report these readings to a healthcare professional weekly for follow-up and treatment evaluation. Goal blood glucose levels for women with GDM can be seen in Table 1.
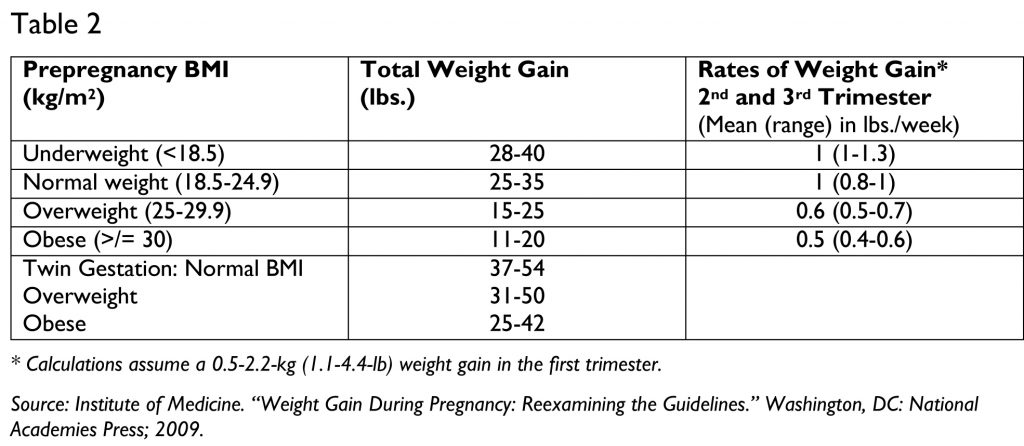
Diet therapy includes a healthy, well-balanced eating plan that is aimed at supporting the pregnancy and promoting blood sugar control. It is recommended that the woman with GDM eat at least 3 meals and 2-4 snacks throughout the day and aim for a variety of nutrients through their food choices. Estimating energy, macro- and micronutrient and fluid needs, and evaluation of growth/weight does not differ from recommendations for pregnant women without GDM. Suggested weight gain during pregnancy can be seen in Table 2. There is no additional need for extra calories during the first trimester, and generally, most women will need to increase their estimated energy requirements (EER) by 340 kilocalories in the second trimester, and by 452 kilocalories in the third trimester. Carbohydrate needs vary depending on the individual. The Recommended Daily Allowance (RDA) for carbohydrate for pregnant women is 175 grams per day to provide glucose for fetal brain development, however, a healthy macronutrient distribution is generally 40-60% of calories from carbohydrate. It is important that pregnant women consume adequate fiber, water, and protein daily, as well as macro- and micronutrients – such as vitamin D, folate, calcium, choline, iodine, and iron.
Pregnant women should be advised to avoid alcohol, uncooked (including deli meat), raw or unpasteurized foods, and certain foods high in mercury content. Women with GDM should limit refined and added sugars to no more than 10% of their caloric needs. They should also avoid trans fats, such as partially hydrogenated oils, as these foods contribute to insulin resistance. Women diagnosed with GDM are encouraged to meet with a Registered Dietitian Nutritionist (RDN) or Certified Diabetes Educator (CDE) in order to develop a healthy eating pattern to be followed throughout the pregnancy.
After Pregnancy
Since having a diagnosis of GDM increases a woman’s risk for developing T2DM later in life, it is important for women to continue following a healthy eating pattern after pregnancy. All women with a diagnosis of GDM should be referred back to their family physician or other health care provider and having an open communication with the delivering provider is important. Women should be evaluated for persistent diabetes or prediabetes 4-12 weeks postpartum with a 2 hour 75-gram oral glucose tolerance test (OGTT), and then every 1-3 years thereafter. The OGTT is recommended over A1C in the 4-12 week postpartum period because the A1C may still be impacted (lowered) by the increased red blood cell turnover during pregnancy or blood loss during delivery. Women should be encouraged to breastfeed as they are able, as this can provide long-term metabolic benefits to the mother and offspring. Women should be encouraged to achieve a healthy body mass index (BMI) postpartum, as postpartum weight gain increases a woman’s chance of developing T2DM. The risk of developing T2DM after a GDM pregnancy is greatest within the first 10 years postpartum.
In the prospective Nurses’ Health Study II (NHS II), diabetes risk after a history of GDM was lower in women who followed healthy eating patterns, including a diet rich in fruits and vegetables, whole grains, lean protein, and low-fat dairy. According to the Diabetes Prevention Program Group research, adding either lifestyle intervention or metformin during the postpartum period is highly effective in reducing a woman’s risk of progression to T2DM.
Special Considerations for Individuals Whose Mother Had GDM
Children born to mothers who had GDM are at greater risk for developing T2DM later in life as well. It is essential for offspring of women who had GDM to follow healthy lifestyle patterns to reduce their own risk for developing diabetes, including following a healthy eating pattern, participating in regular exercise, and achieving and maintaining a healthy weight.
Conclusion
Although uncontrolled blood sugars can lead to many serious complications, there are many things a woman can do to promote glycemic control. It is paramount that women of all stages of life evaluate their lifestyle choices and avoid habits that lead to insulin resistance. Women should receive education from their primary care team to encourage prevention of insulin resistance, and should be screened appropriately to address issues as they arise. While GDM can be an overwhelming diagnosis for many, providing support and treatment can help women to manage this disease and give them the confidence to be advocates for their own health.
References available on the OAFP website.